
Choosing between veneers and dental implants can feel overwhelming for patients who aren’t completely savvy with their choices, especially when you just want a healthy, confident smile. Both options can transform the way your teeth look, but they work in very different ways and suit different situations. In this article, we will walk you through what veneers and implants are, how they differ, and how the team at Gisborne Family Dental can help you decide what is right for you.
How veneers work
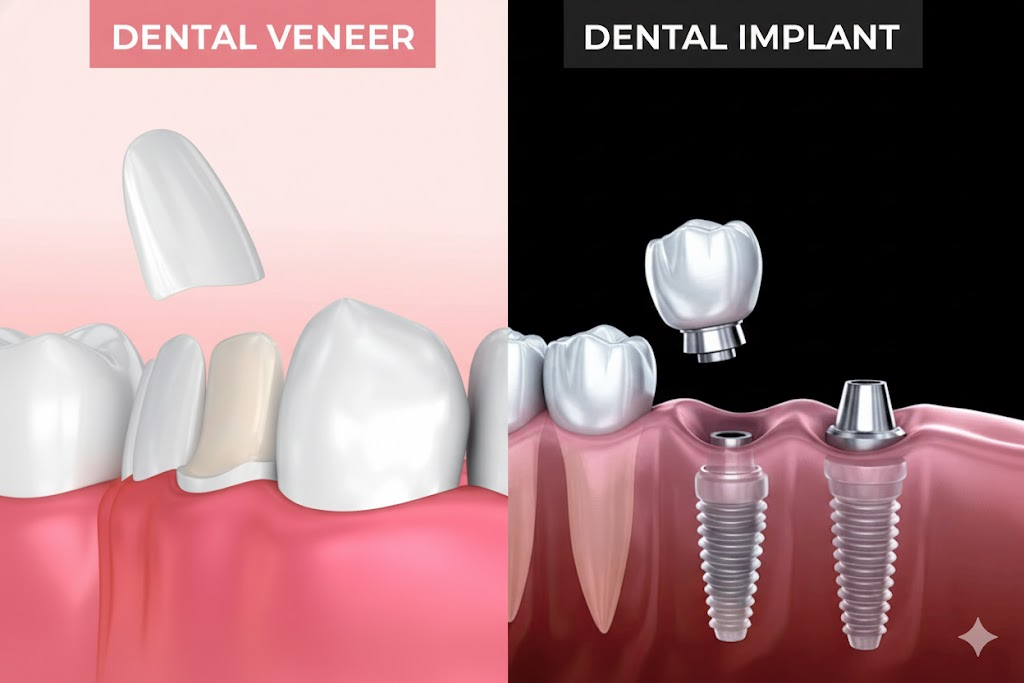
Veneers are thin shells that are bonded to the front surface of a tooth to change how it looks. They are usually made from porcelain or composite resin.
From a clinical point of view, traditional porcelain veneers involve a small amount of tooth preparation. In most cases, about 0.5 to 0.7 millimetres of enamel is removed from the front of the tooth, which is roughly the thickness of a fingernail, so that there’s room to bond the veneer without adding unflattering bulk to the tooth front
Key steps usually include:
- Assessment of the tooth and surrounding tissues
- Careful preparation of the enamel, usually kept within enamel to protect the tooth and support bonding
- An impression or digital scan to design the veneer
- Try in and adjustment of the veneer
- Final bonding and polishing
Minimal prep or no prep veneers may use even thinner porcelain, sometimes around 0.2 to 0.5 millimetres, which can reduce or avoid the need for enamel removal in selected cases.
Veneers are generally used when:
- The tooth is present and structurally sound
- The concern is colour, minor shape issues or small gaps
- There is no need to replace the root or the whole tooth
How dental implants work
Dental implants are used to replace missing teeth, or teeth that cannot be saved. An implant replaces the root, and then supports a crown, bridge or denture.
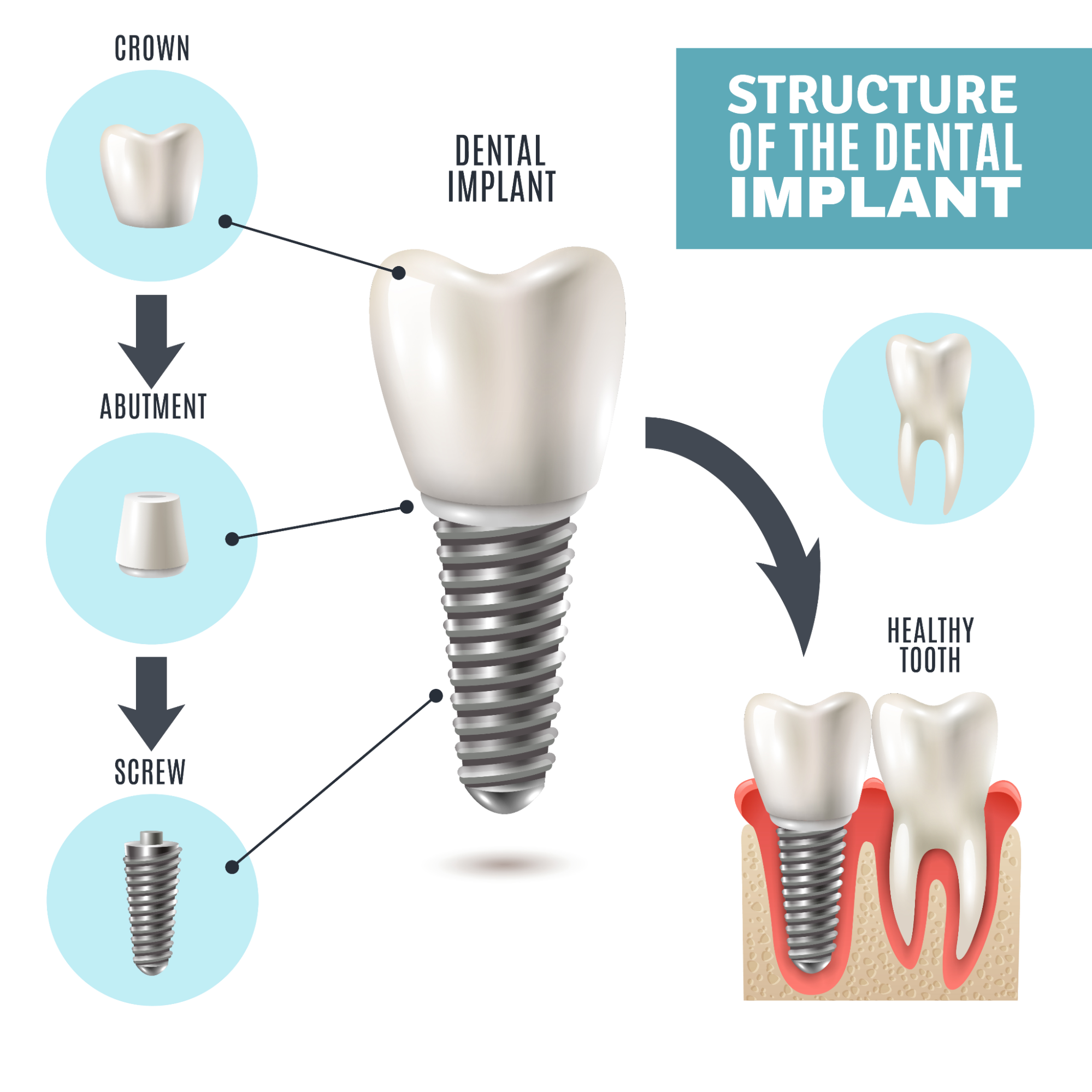
A standard single implant has three parts:
- A titanium fixture placed into the jaw bone
- An abutment that connects the fixture to the restoration
- A crown that appears above the gum and looks like a tooth
Treatment usually occurs in stages:
- Planning with clinical examination and imaging such as X rays or CBCT
- Placement of the implant into the bone under local anaesthetic
- Healing phase, often several months, while bone integrates with the implant
- Restoration, where an abutment and crown are fitted and adjusted
Modern implant systems show high survival rates. Many studies report around 90 to 95 per cent survival at 10 years, and some report function extending beyond 20 years when cases are well planned and maintained.
Implants are generally preferred when:
- A tooth is missing or needs to be removed
- The patient wants a fixed option rather than a removable denture
- There is enough healthy bone, or bone can be augmented
From a clinical point of view, the starting question is simple: is the tooth still restorable or not?
If the tooth is present, structurally sound and free of severe cracks or infection, veneers and other conservative options can usually be considered. If the tooth is missing or cannot be predictably restored, replacement options such as implants come into the picture.

When assessing a tooth, dentists typically look at:
- Tooth structure
- Is there enough healthy enamel and dentine left to support a veneer or crown?
- Has the tooth had large fillings, root canal treatment or fractures below the gum line?
- Gum and bone health
- Are the gums stable, with no untreated periodontal disease?
- Around implants, long term success depends on having enough healthy bone and low inflammation.
- Poorly controlled gum disease increases the risk of both veneer failure and implant complications.
- Bite and function
- Are there heavy bite forces, clenching or grinding (bruxism)?
- Veneers on patients with strong grinding habits can chip or debond more often.
- Implants in very heavy bite situations may need careful design, night splints or alternative options.
- Aesthetic goals
- Is the concern one or two teeth, or the entire visible smile line?
- Veneers can be planned in sets (for example 4, 6 or 8 teeth) to create a harmonised appearance.
- An implant crown must blend with neighbouring teeth in shape, colour and gum line.
- Time and tolerance for treatment
- Veneers often involve fewer appointments and no surgical phase.
- A single implant can involve several months from placement to final crown, especially if bone grafting is required.
- Some patients strongly prefer to avoid surgery, while others prioritise a fixed replacement over a removable option.
- Cost over a lifetime
This is not just the initial fee for veneers or implants. It includes how long each option lasts, how often it needs replacement and any extra treatment required along the way.
- Veneers usually cost less at the start, but they often need to be replaced every 7 to 15 years. Some last longer, but others may fail sooner if the bite is heavy or the underlying tooth changes. Each replacement involves new laboratory work, new bonding and careful colour matching. If someone has 4, 6 or 8 veneers, the long term cost increases because replacing one can mean adjusting neighbouring veneers to keep the smile consistent.
- Implants cost more upfront because they involve planning, surgery and a custom crown. However, the implant fixture itself can last decades. Most research shows around 90 to 95 per cent survival at 10 years when maintained well. What usually needs replacement is the implant crown, often after 10 to 15 years, which is generally less costly than replacing multiple veneers.
- Over 20 to 30 years, a single veneer can be cheaper than an implant if the tooth is strong and stable. For missing teeth, a single implant often becomes more cost effective than repeated removable options or multiple veneer cycles.
In many cases, both options are not truly interchangeable. For example, a missing upper front tooth is usually better restored with an implant, bridge or denture rather than a veneer, because there is no tooth left to bond to. On the other hand, a discoloured but solid front tooth is often better treated with a veneer or crown rather than extraction and implant placement.
From a clinical point of view, veneers and dental implants are very different tools. Veneers are usually used to improve the appearance of teeth that are still present and structurally sound. Implants are used to replace teeth that are missing or cannot be predictably restored.
There is no single option that is “better” for everyone. The most suitable treatment depends on:
- The condition of the tooth and surrounding bone
- Your bite, jaw joints and any grinding or clenching
- Your medical history and gum health
- How many teeth are involved and where they sit in the smile
- Your expectations about appearance, time and maintenance
A thorough examination allows a dentist to explain which options are realistic in your case, along with the likely benefits, risks and long term outlook for each.
When discussing veneers or implants with a dentist, it can be helpful to ask:
- What are all the reasonable options for this tooth or area?
- How long is each option expected to last in my situation?
- What maintenance will I need over time?
- What are the main risks or limitations of each option for me?
Veneers may NOT be suitable if:
- There is active bruxism without management
- Enamel is severely worn or missing
- Gum recession creates uneven margins
- The tooth is severely rotated or misaligned (orthodontics may be needed first)
Implants may NOT be suitable if:
- Bone volume is insufficient and grafting is declined
- Uncontrolled diabetes
- Immunosuppressive conditions
- Smoking more than 10–15 cigarettes a day
- History of bisphosphonate or anti-resorptive therapy (risk of osteonecrosis)
The goal is to choose a treatment that does more than change how teeth look. Ideally it should support long term oral health, feel comfortable in function and fit well with your general health and lifestyle.


